Re-do endovascular endoleak embolisation by transprosthetic puncture after endovascular aneurysm repair
Explore the complex case of a 71-year-old male with a history of multiple aortic aneurysm repairs, now presenting with a large Type II endoleak. This patient’s evolving condition challenges the management of aneurysms with recurring endoleaks despite previous interventions.
Dive into the full clinical presentation and imaging to see the progression of his condition and weigh in on the treatment options in our interactive poll!

Reminder
- Type I endoleak (attachment site)
- Type II endoleak (branch)
- Type III endoleak (graft failure)
- Type IV endoleak (porosity)
- Endotension (no visible endoleak)
Type II Endoleak
Incidence: 24 %;
Treatment:
- Trans-arterial;
- Trans-lumbar;
- Trans-caval;
- Trans-abdominal;
- Microcatheter;
- Laparoscopic ligation;
Materials: coils, glue, thrombin, plug, stent (anchoring technique);
71-year-old male patient hospitalised at Clinique Pasteur, Toulouse, in June 2024, for the management of a Type II endoleak
Cardiovascular risk factors:
- Hypertension
- Dyslipidemia
AAA history
- 2018: AAA 52 mm → bifurcated aortic endoprosthesis;
*Type II endoleak between the superior mesenteric artery and the inferior mesenteric artery. - 2020: AAA 55 mm → embolisation of aneurysmal sac and inferior mesenteric artery with coils;
*Complete embolisation of mesenteric artery, type II endoleak through a renal collateral circuit. - 2022: AAA 64 mm → ligation of the left inferior polar artery was considered;
- 2023: AAA 70 mm → direct injection of Onyx through a scan-guided percutaneous puncture;
- 2024: AAA 80 mm → large Type II endoleak (unclear on CT imaging)
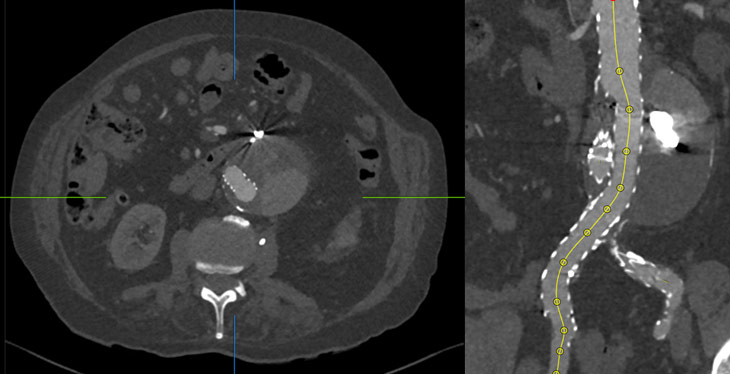
- Right common femoral approach evidence of ilio-lumbar endoleak, with no evidence of Type I or III endoleaks.
- Direct needle puncture on the right iliac branch (BRK™ Transseptal Needle - Abbott).
- Embolization with multiple 20 x 39 mm coils (Terumo).
- 16 x 16 x 124 mm covered endoprosthesis on the right iliac leg (optimisation by AB46).
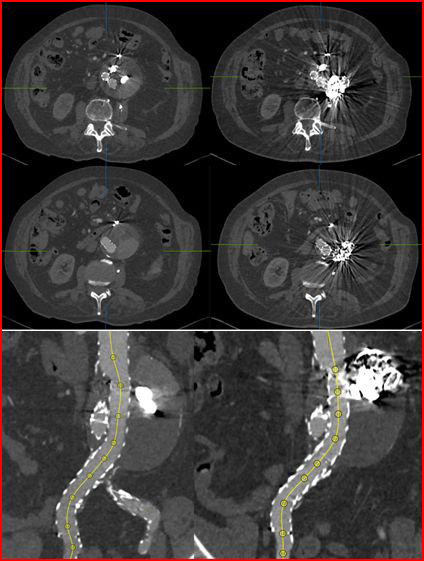
Post-operative period uneventful, with no local or general complications
Metallic artifacts prevent the detection of any potential persistence of the leak between the coils.
At control CT, the coils were positioned in the same location where the endoleak was visible in the pre-procedural CT.
Get the latest clinical cases and breaking news delivered straight to your inbox!
