Transprosthetic embolization
Would you be able to determine the most effective treatment plan for a 73-year-old patient whose aneurysm sac has enlarged after two years of stability post-endovascular repair of an abdominal aortic aneurysm? Examine this clinical case and contrast your treatment approach with that of your peers!

Professor of vascular surgery
Head of unit of vascular surgery CHU Bordeaux - France
Conflicts of interest:
Honoraria from: COOK Médical, Térumo-Vascutek, Siemens, GORE
- The patient is a 73-year-old man
- He has a medical history of high blood pressure
- 2020: previous Anaconda EVAR (EndoVascular Aneurysm Repair) for AAA (Abdominal Aortic Aneurysm) 62 mm treatment
- 2020-2022: aneurysmal sac stability with type 2 endoleak ; AAA diameter 44 mm (vs 62 mm before surgery)
- Since February 2023, an enlargement of the aneurysm sac has been observed, at a rate of + 5 mm in one year.
- The chosen option is transgraft direct embolization
- To carry out this procedure, here is the list of required material:
- Steerable sheath 7 Fr
- Needle Catheter
- Stiff 0.018 guidewire
- Coils
- Glue
- Planned way and devices used:
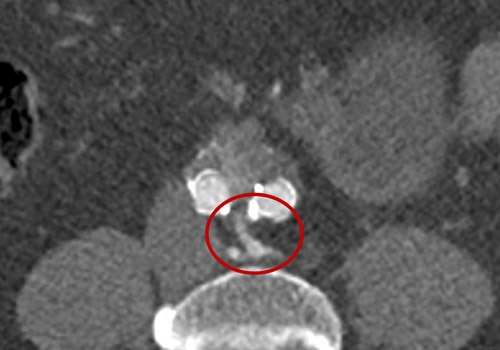
- A transprosthetic puncture was performed using a BeBack® (Bentley) 360° rotating crossing catheter.
- A specific stiff 0.018 ThruwayTM guidewire (Boston Scientific) was also used.
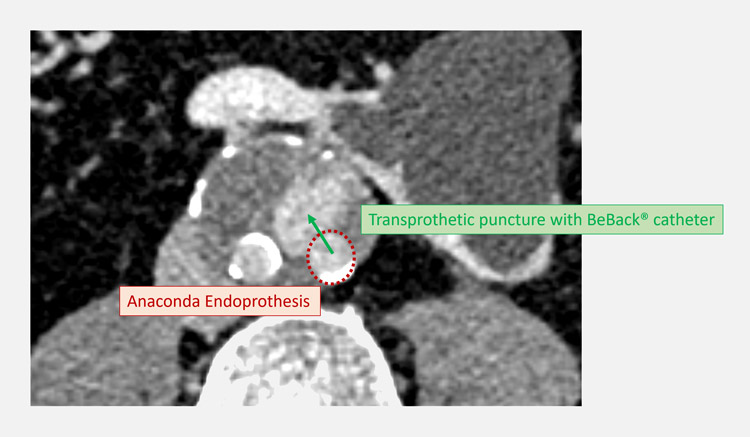
Description of the BeBack® catheter with 0.018 distal needle, used (+/- with a 7 Fr steerable catheter) to puncture and perforate the graft in order to reach the liquid in-sac phase.
Beginning of the embolisation... It is necessary to fill until the liquid phase is complete.
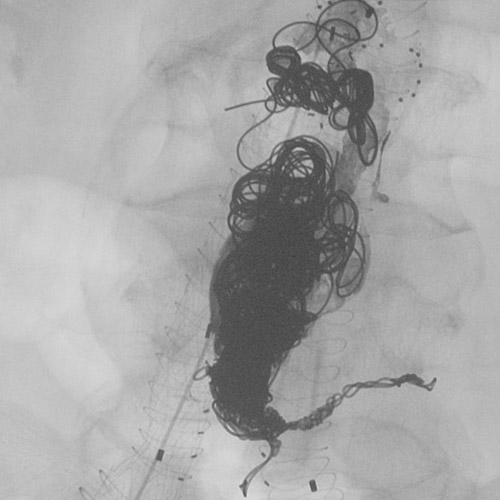
21 coils later... The use of glue (Onyx™ liquid embolic system) is crucial to completely fill the liquid phase and stop the diffusion and circulation of blood.
The procedure should be completed by closing with a leg endoprosthesis (Gore® PLC161000).

Final result: lumbar arteries with liquid space completely coiled and filled with glue.
Follow-up
- It is crucial to carefully follow up the treated patient with a US duplex at 6 months and an AngioCT scan at 1 year, with maximum diameter and global volume determination and comparative evaluation.
- Advantages of this technical aspect:
- Direct access to the liquid phase and in-sac navigation to determine and reach the inflow and outflow arteries
- Selective inflow (+/- outflow) embolization + complete liquid space coiling and filling with large glue administration and diffusion.
Get the latest clinical cases and breaking news delivered straight to your inbox!
