Treatment for no-option CLTI patient
In the past decade, patients affected by chronic limb-threatening ischemia (CLTI) have increased, mostly due to a rise in population age and diabetes. In about 15-20 % of CLTI patients, arterial revascularisation is not possible, or not effective (no-option). Severe MAC-score is an independently factor of redo-treatment, persistent ischemia and major amputation, despite a successful arterial revascularisation.

A 79 year-old male patient
Comorbidities:
- arterial hypertension;
- type 2 diabetes;
- atrial fibrillation
- chronic renal disease (GFR 31 ml / min)
Foot presentation
- Right foot: previous amputation of the first toe and metatarsal bone for wet gangrene (in another hospital, without revascularisation)
- Necrosis of the surgical site due to the CLTI (TcpO2 = 3 mmHg)
- WIfI class = 2-3-1

Quiz answer
Timing: revascularisation before, foot surgery after
Surgical/endovascular arterial revascularisation is the first treatment choice in case of CLTI, in order to increase oxygen and nutrition in the ischemic area.
Treatment choice
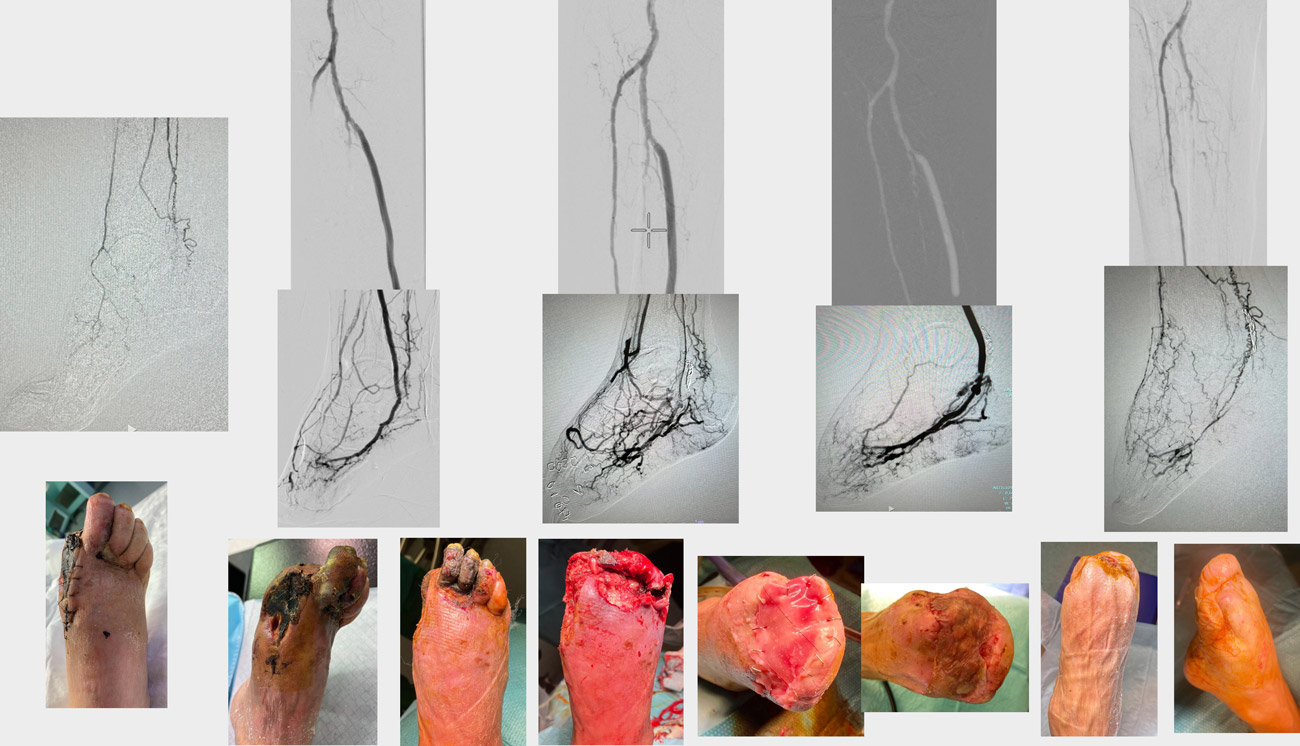
Angiography: patency of the anterior tibial, but occlusion of the dorsalis pedis; patency of peroneal; occlusion of posterior tibial
Foot X-ray: diffuse calcification in the foot arteries (MAC-score = 5)
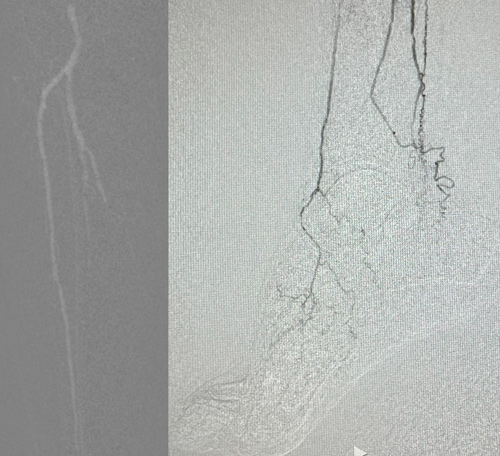
Due to the presence of severe MAC score and no distal artery for bypass surgery, the treatment choice is foot venous arterialisation.
Based on the angiography, percutaneous-DVA could be considered the first choice, because arterial flow into the foot is supplied by the anterior tibial and peroneal arteries
“STORM” after p-DVA
- Cyanosis
- More pain
- Extension distal necrosis
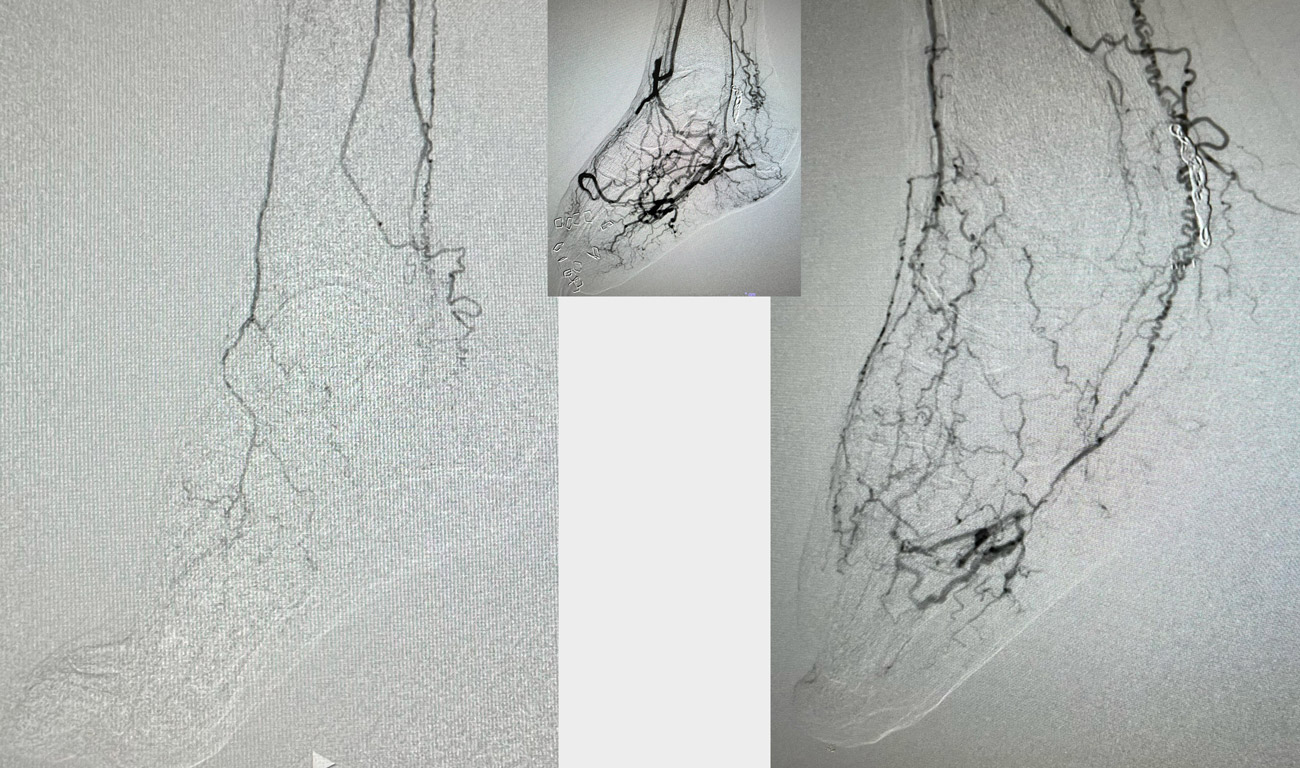
Flow focalisation
Coil embolisation is done to reduce the stealing of blood

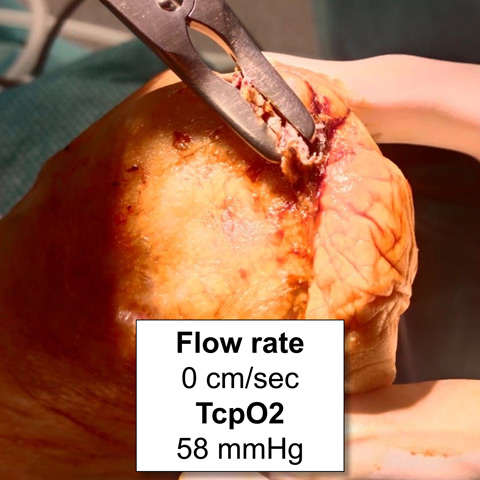
Tension-free surgery
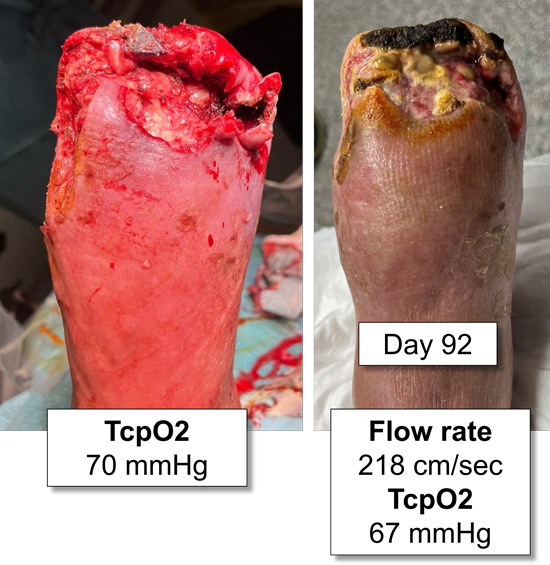
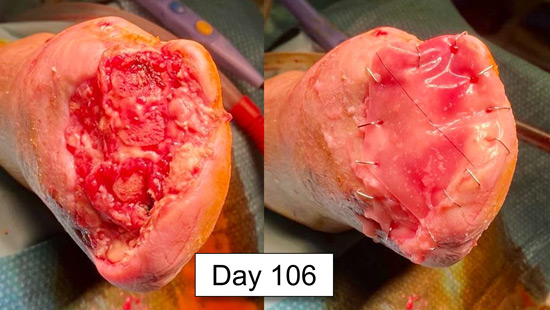
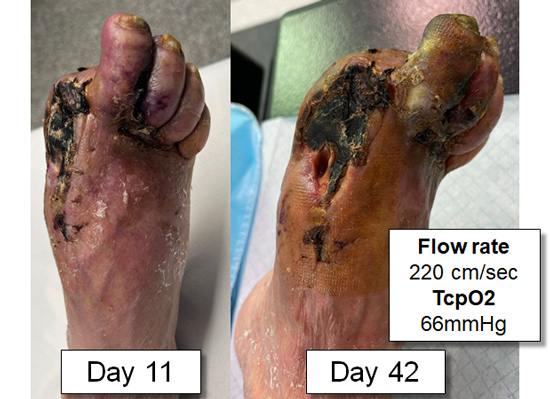
Progressive maturation of arterialised circuit

Wound recurrence
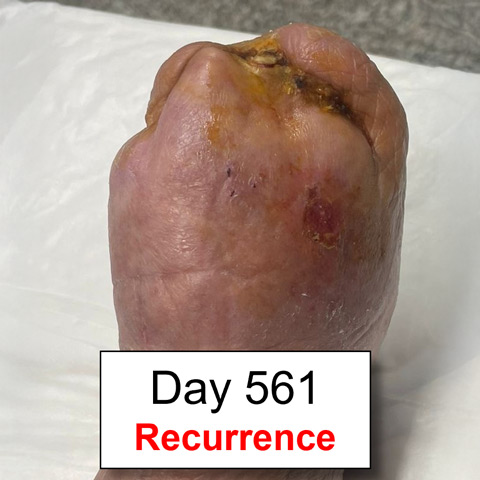

Despite p-DVA occlusion, a new network of arteries allowing continuous perfusion
Get the latest clinical cases and breaking news delivered straight to your inbox!
