IVUS-guided vs angiography-guided drug-coated balloon angioplasty in patients with complex femoropopliteal artery disease
Selected in JACC: Cardiovascular Interventions by Clément Cui
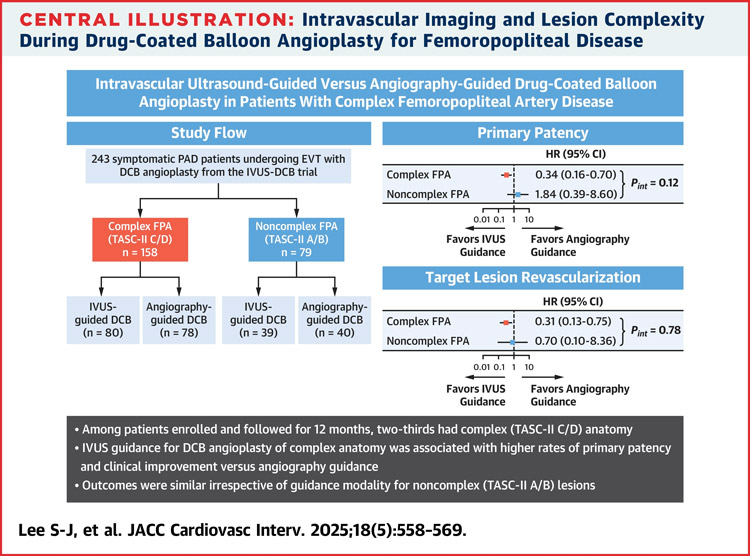
This publication review focuses on a subgroup analysis of the randomised IVUS-DCB trial, which explored whether intravascular ultrasound (IVUS) guidance offers clinical advantages over traditional angiography in drug-coated balloon (DCB) angioplasty for femoropopliteal artery (FPA) disease.
Among 257 patients — including 158 with complex lesions — IVUS guidance was associated with significantly better 12-month outcomes in the complex group: higher primary patency rates, lower CD-TLR, and more sustained clinical and hemodynamic improvements. Interestingly, in patients with non-complex FPA, no significant benefit was observed.
Explore the data and understand how imaging guidance could reshape your endovascular strategy.
References:
Authors: Seung-Jun Lee, Tae-Hoon Kim, Jae-Hwan Lee, Chul-Min Ahn, Sang-Hyup Lee, Yong-Joon Lee, Byeong-Keuk Kim, Myeong-Ki Hong, Yangsoo Jang, Ha-Wook Park, Ji Yong Jang, Jae-Hyeong Park, Su Hong Kim, Eui Im, Sang-ho Park, Donghoon Choi, Young-Guk Ko, and the IVUS-DCB Investigators
Reference: J Am Coll Cardiol Intv. 2025 Mar, 18 (5) 558–569
DOI: DOI: 10.1016/j.jcin.2024.10.052
Read the abstractBackground:
Endovascular procedures are still predominantly performed under angiographic guidance. While widely used, angiography only provides two-dimensional imaging and involves significant radiation exposure. Intravascular ultrasound (IVUS) offers important advantages, including three-dimensional visualisation, detailed assessment of plaque characteristics (size, composition), and precise guidance device positioning. However, IVUS comes with added cost and requires additional time and effort from the operator, making its widespread use across all procedures challenging. This raises an important question: which femoropopliteal lesions benefit most from IVUS guidance?
Objective:
To compare the clinical impact of IVUS-guided vs angiography-guided drug-coated balloon (DCB) angioplasty in patients with complex or non complex femoropopliteal lesions
Methods:
- Subgroup analysis of the randomised IVUS-DCB trial
- Patients with FPA undergoing DCB angioplasty were randomised to receive the procedure under IVUS or angiography guidance
- The primary endpoint was 12-month primary patency.
Outcomes:
- 257 patients : 158 complex FPA / 79 non-complex FPA
- Complex FPA : IVUS guidance was associated with significantly higher rates of primary patency, freedom CD-TLR and sustained clinical and hemodynamic improvement relative to angiography guidance
- Non-complex FPA : no significant difference in primary patency

Get the latest clinical cases and breaking news delivered straight to your inbox!

Discussion:
This study highlights the benefit of IVUS guidance over angiography in DCB angioplasty for complex femoropopliteal lesions (TASC C/D), with improved primary patency and reduced reintervention rates.
IVUS was especially effective in long, calcified, or occlusive lesions, and in cases of critical limb ischemia. However, these lesion types often require stenting due to frequent dissections, and the efficacy of DCB is reduced in very long or heavily calcified lesions.
Accurate vessel sizing with IVUS—based on external elastic lamina—may explain improved outcomes, though it can lead to device oversizing.
While the study had independent blinded evaluation, limitations include open-label design, operator dependency of IVUS, lack of standardised vessel preparation, and CT-based follow-up instead of duplex ultrasound.
Conclusion:
In endovascular treatment of FPA using DCB, IVUS guidance was significantly associated with improved 12-month clinical outcomes, particularly in patients with complex FPA lesions.