Branched stent-graft used for type IV thoracoabdominal aneurysm in abdominal aortic agenesis
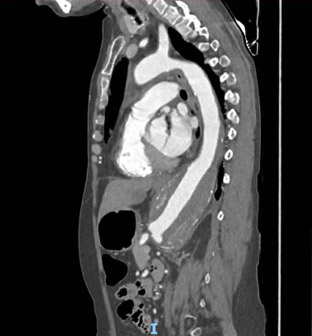
This case report considers a 49-year-old women which presented a progressive large aneurysm of the type IV thoraco-abdominal aorta in a context of abdominal aortic agenesis.
In collaboration with:
C. Caradu, J. Pudzeis - Dept of Vascular Surgery, CHU Pellegrin, Bordeaux, France
M. Pernot, A. Aguettant d'Aubigny, L. Labrousse - Dept of Cardio-thoracic Surgery, CHU Haut-Lévêque, Bordeaux, France

Professor of vascular surgery
Head of unit of vascular surgery CHU Bordeaux - France
Conflicts of interest:
Honoraria from: COOK Médical, Térumo-Vascutek, Siemens, GORE
- Active smoking
- Arterial hypertension
- Abdominal aortic agenesis
- Solitary functioning right kidney
- Left transfemoral amputation at 35 and right transtibial amputation at 37 in a context of arterial thrombosis
- Pulmonary embolism at 18
- Peripartum deep vein thrombosis
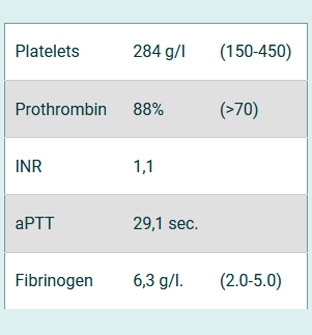
Thrombophilia suspected
- Weight : 40kg
- Height : 140cm (<165cm)
- GFR : 74,6 ml/min
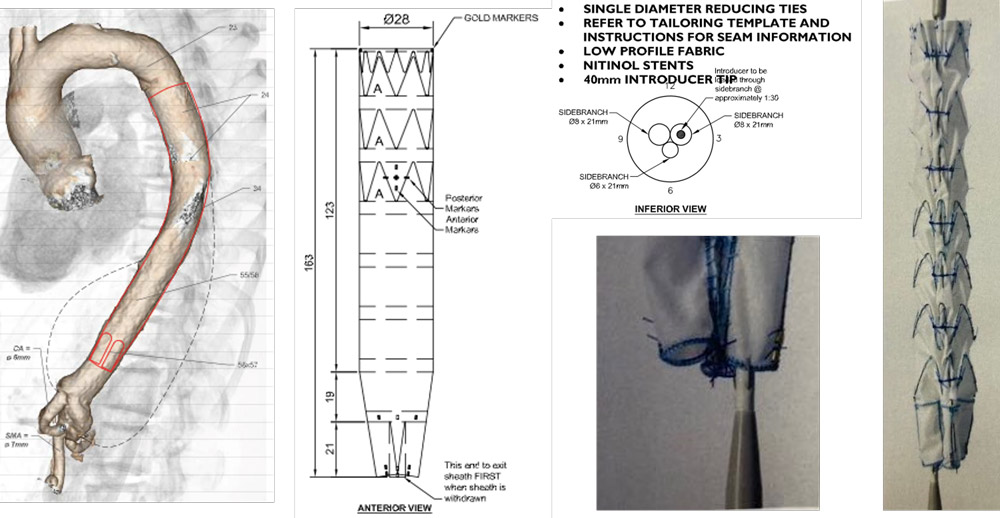
Custom-made triple-branched endovascular graft (Cook Medical) deployed from a trans-apical access
Angiogram perioperative
Trans-apical access by anterior thoracotomy
- Transoesophageal echocardiogram control
- Hybrid suite with fusion imaging capabilities
- Heparinization systemic

Stenting of the target vessels by right axillary artery
- 8Fr introducer
- Covered stents (COVERA™ BD)
- RRA: 7mm diameter
- CT: 9mm diameter
- SMA: 8mm diameter
ACT : 238-240 seconds
Post operative period
Total thrombosis of the stent-graft and mesenteric portal veinous system
- Prosthetic bypass between ascending aorta and right hepatic, SMA and right renal arteries
Multiple complications
- D+2 Haemostasis for haemorrhage, right colectomy and cholecystectomy
- D+4 Making of an ileocolostomy, 60cm resection of necrotic bowel, evacuation of hematoma of the mesentery
- Persistant thrombocytopenia (Platelets 7 g/l) of multi-factorial origin (peripheral consumption on multiple thromboses, splenomegaly on portal thrombosis, inflammation, spinal stupor)
- Kidney failure KDIGO 3 dialysis
- Grade E pancreatitis
- Digestive bleeding (peristomial, gastric ulcers)
- D+12 MOF and died
Discussion
Agenesis of the abdominal aorta and iliac arteries is an extremely rare congenital vascular anomaly, associated with various long-term morbidities.
To treat thoracoabdominal aortic aneurysm, open procedures are more complex and associated with high mortality and morbidity rates
In the presented case, the patient was evaluated in a multidisciplinary team. High risk of pelvic necrosis under ECC and under-recognized or misdiagnosed hemophilia contraindicated open repair. An endovascular repair was considered to be the optimal solution.
The absence of an adequate femoral or iliac access to deliver a branched or fenestrated endograft is usually considered an absolute contraindication for endovascular repair.
Alternative routes and dedicated stent-graft designs have been advocated.
- Transapical and axillary access to deploy standard straight thoracic stent-grafts has been previously demonstrated in patients with aorto-iliac occlusion
Malik, K., Poletto, G., Zhao, Y., & Civilini, E. (2019). Unconventional Endovascular Access for Symptomatic Thoracic Aortic Ulcer with Infrarenal Aortic Occlusion—A Case Report. Annals of Vascular Surgery. - Only one other case use of a custom-made triple- branched endovascular graft deployed from a transaxillary access to treat a aneurysm associated with pararenal aortic occlusion
- Postoperative course was uneventful
Bertoglio, L., Lopes, A. C., Rinaldi, E., Bossi, M., Berchiolli, R. N., Ferrari, M., & Chiesa, R. (2022). Transaxillary Tri-Branch Aortic Endovascular Graft Repair of Recurrent Thoracoabdominal Aneurysm With Pararenal Aortic Occlusion. Journal of Endovascular Therapy
Conclusion
The use of this custom-made tri-branched device, combined with the transapical access, allowed to treat this aneurysm through a less invasive approach, despite the unfortunate outcome.
Transapical and axillary access have allowed to extend the number of eligible patients to endovascular approach.
Further validation and longer follow-up times would be required to prove the effective durability of this visceral aortic stump
- Post operative anticoagulation management more aggressive?
References
- Bertoglio, L., Lopes, A. C., Rinaldi, E., Bossi, M., Berchiolli, R. N., Ferrari, M., & Chiesa, R. (2022). Transaxillary Tri-Branch Aortic Endovascular Graft Repair of Recurrent Thoracoabdominal Aneurysm With Pararenal Aortic Occlusion. Journal of Endovascular Therapy. 152660282211026.
- Helmy, A., Catarino, P., Dunning, J. H., Hayes, P. D., Goon, S., & Winterbottom, A. (2018). Branched Thoraco-Abdominal Aortic Aneurysm Repair with Branch Access Through a Transapical Left Ventricular Approach. CardioVascular and Interventional Radiology.
- Malik, K., Poletto, G., Zhao, Y., & Civilini, E. (2019). Unconventional Endovascular Access for Symptomatic Thoracic Aortic Ulcer with Infrarenal Aortic Occlusion—A Case Report. Annals of Vascular Surgery.
Get the latest clinical cases and breaking news delivered straight to your inbox!
