Management of a type II endoleak after thoraco-abdominal aneurysm endovascular exclusion
A 73-year-old man with multiple cardiovascular risk factors presented with acute thoraco-abdominal pain and was found to have a large thoraco-abdominal aneurysm associated with bilateral iliac aneurysms.
To limit the risk of spinal cord ischemia, a staged endovascular strategy was planned, combining TEVAR, a branched endograft with visceral vessel stenting, and bilateral iliac branch repair.
Despite the complexity of the procedure and embolisation of the celiac trunk, follow-up imaging at 6 months revealed a persistent type II endoleak with aneurysm sac enlargement, raising the question of optimal secondary management.



- A 73-year-old male patient
- Anamnesis: heavy smoker, hypertension, diabetes, dyslipidemia and chronic obstructive pulmonary disease
- Acute chest, abdominal and lumbar pain
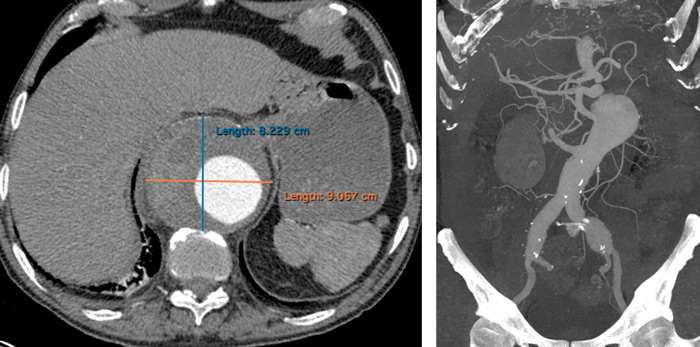
- Urgent CT scan: voluminous thoraco-abdominal aneurysm and bilateral iliac aneurysm

Planning
Due to the extension of the disease, to reduce the risk of spinal cord ischemia, we planned a multistage procedure:
- TEVAR (thoracic endovascular aortic repair)
- Deployment of a T-branch endograft with left renal artery and superior mesenteric artery stenting
- Bilateral iliac branch
- Stenting of right renal artery and celiac trunk
Technical drawing
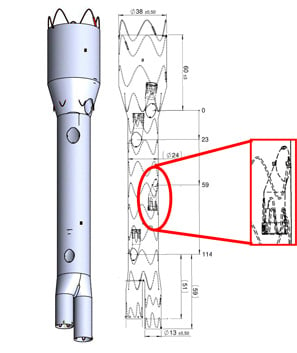
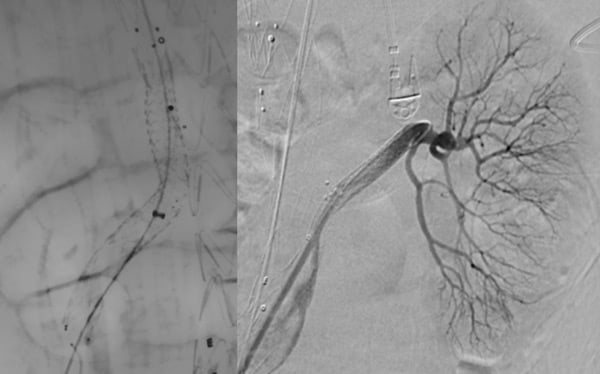
Step 1: TEVAR


Step 2: SMA and LRA stenting
(30 days after step 1)
Step 3: bilateral iliac branch
(45 days after step 2)

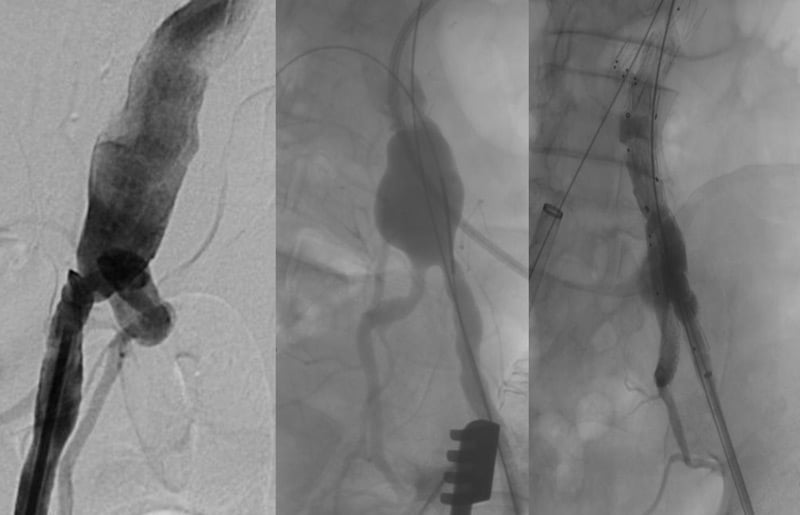

Step 4:
(30 days after step 3)
- RRA stenting
- Celiac trunk
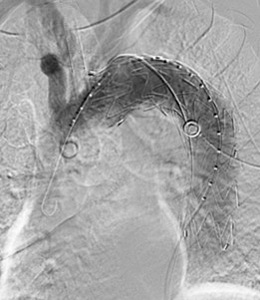
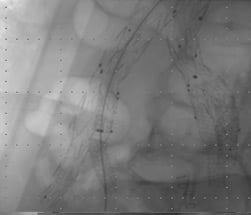
Cannulation
Failure
↓
- Celiac trunk
Branch
Embolisation


Follow-up
At CT scan control, 6 months after operation, the patient had a type-2 endoleak with enlargement of the aneurysmal sac.
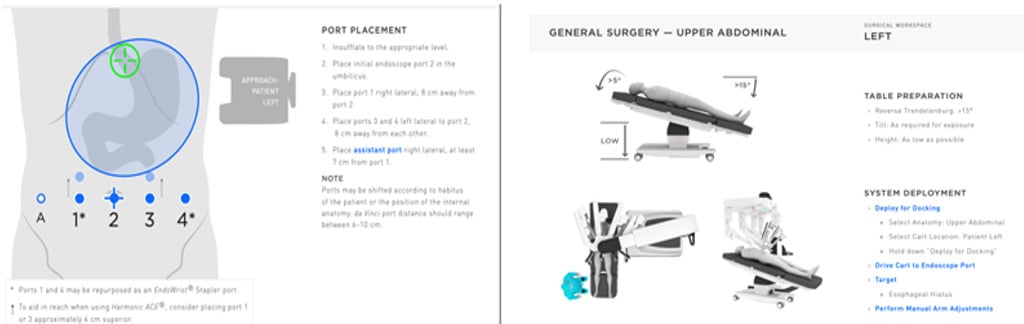
- After pneumoperitoneum induction, the flaccid part was opened and splenic, left gastric and hepatic arteries were identified and carefully isolated.
- The vessels were temporary clamped and green indocyanin was injected to exclude visceral ischemia.
- So, finally, the celiac trunk was closed with a clip at its origin from the aorta.
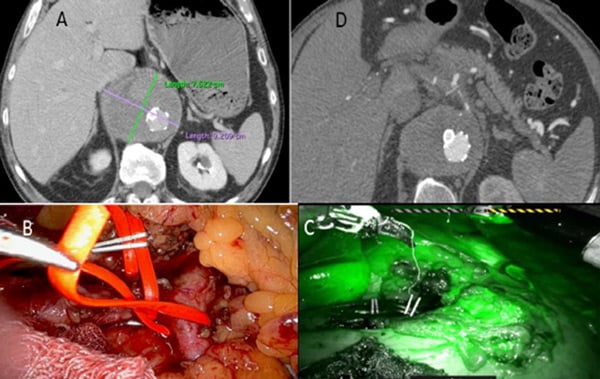
Robotic celiac trunk ligature
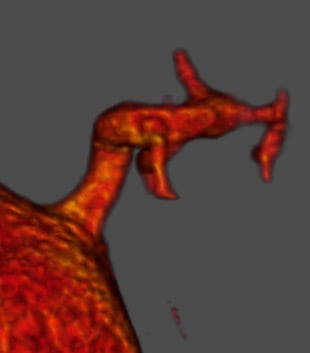
- Type II endoleak (A);
- Celiac branches temporary robotic clamping (B);
- Check with indocyanin green injection (C);
- Type II endoleak complete resolution after celiac trunk ligature (D).
CT-scan follow-up
- Complete type II endoleak resolution
- Absence of visceral ischemia
- No spinal cord ischemia

Conclusions
- Type II endoleak is very frequent after endovascular abdominal aortic aneurysm repair, but its incidence is underinvestigated after endovascular exclusion of a thoraco-abdominal aneurysm.
- Usually, it is followed up and treated only in cases of aneurysmal sac enlargement.
- The celiac trunk robotic ligature is minimal invasive and can offer excellent results.
- The current literature reports some cases of inferior mesenteric artery or lumbar arteries robotic ligature, but celiac trunk robotic ligature to treat type II endoleak has never been reported to date.
Total robotic ligation of inferior mesenteric artery for type II endoleak after endovascular aneurysm repair.
Lin JC, Eun D, Shrivastava A, Shepard AD, Reddy DJ.
Ann Vasc Surg. 2009 Mar;23(2):255.e19–21.
doi: 10.1016/j.avsg.2008.02.019. Epub 2008 Apr 14.
PMID: 18411030
Technical details and preliminary results of a full robotic type II endoleak treatment with the da Vinci Xi.
Morelli L, Guadagni S, Di Franco G, Palmeri M, Furbetta N, Gianardi D, Bianchini M, Moglia A, Di Candio G, Ferrari M, Berchiolli R.
J Robot Surg. 2019 Jun;13(3):505–509.
doi: 10.1007/s11701-019-00944-z. Epub 2019 Mar 4.
PMID: 30830571
Indocyanine green colonic perfusion demonstration following robotic da Vinci X inferior mesenteric artery ligation for the treatment of type II endoleak.
Lambert J, Al Majid S, Salaman R, Gavan D, Sheikh A, Gill M.
Int J Med Robot. 2022 Aug;18(4):e2407.
doi: 10.1002/rcs.2407. Epub 2022 Apr 23.
Get the latest clinical cases and breaking news delivered straight to your inbox!
