Carotid
CAS
Severe carotid artery stenosis associated with contralateral carotid occlusion
In this case, a 72-year-old man with an extensive history of cardiovascular interventions is admitted for supra-aortic trunk angiography after duplex ultrasound revealed sub-occlusion of the right internal carotid artery and critical stenosis of the left.
The challenge lies in determining whether endovascular revascularisation is suitable, and if so, which embolic protection device and stent would be the safest and most effective choice!

Cotignola, Italy

Part I - Case presentation
The patient is a 72-year-old male.
CVRF: obesity (BMI 34,06 Kg/m2), HTN, former smoker, T2DM
Medical history:
- CAD → PCI (w/DES) of right coronary artery (2014)
- 2018 → PTA (w/stent) of right and left iliac axes, and PTA of left SFA
- 2024 → PTA (w/stent) of left common iliac artery and PTA of the left fem-pop axis
- April 2025 → Supra-aortic trunks duplex ultrasound → sub-occlusion of RICA and critical stenosis (80 %) of LICA.
Admitted at our institution for supra-aortic trunks angiography
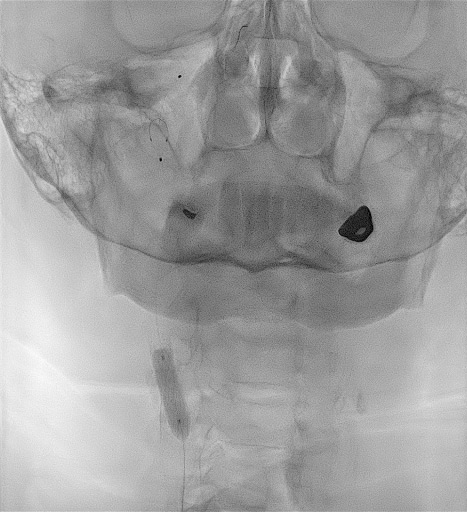
Supra-aortic trunks angiography

Type 1 aortic arch
Slow left hemisphere circulation with contralateral and posterior compensation
Functional occlusion of LICA partially compensated through slow antegrade flow and LECA flow
Right carotid axis
Severe bulb calcification, severe calcified stenosis of the RICA, and pseudo-occlusion of RECA. Severe tortuosity of right internal carotid distally to stenosis
Part II - Final strategy
Lesion wiring and filter positioning
RICA stenosis wiring with two choice floppy (BSCI) wires. Two floppy wires increase support, but the floppy structure of the wire does not straighten the severe tortuosity of the artery
Advancement of 7.0 mm Spider Filter EPD with one floppy buddy wire
Predilation and stenting
Pre-dilatation with NC balloon (3.0 - 20 mm) and Wolverine Cutting Balloon (BSCI) 4.0 x 10 mm
Check after dilatations and removal of the floppy buddy wire
XAct 10 / 10-30 mm
Post-dilation and final result
Post-dilation with 5.5 – 20 mm balloon
To summarise…
- This very complex case was suitable for endovascular treatment, as it was possible to safely treat it with carotid stenting and embolic protection device;
- An embolic protection device is pivotal in carotid stenting, and we never do without it.
In this case, the tight stenosis of RECA was considered a contraindication to Mo.Ma and we used Spider filter; - In this severely calcified, short and subocclusive stenosis, we decided to use a high radial force stent: XAct stent by Abbott Vascular
Get the latest clinical cases and breaking news delivered straight to your inbox!
