Superior Vena Cava Syndrome in patient with ESRD, severe PAD and exhaustion of vascular access options
Investigate this 57-year-old patient's medical history and CT scan, and indicate what you feel is the best option for treating his case.

- 57-year-old male patient with history of previous hemodialysis access induced distal ischemia (HAIDI)
- Severe PAD – previous toe amputations
- Bilateral chronic upper extremity venous outflow problems
- Had a left arm axillary loop graft that was successfully used for a couple of months with minor to moderate left arm swelling.
- While this was initially well tolerated and allowed the removal of the femoral catheter, the patient subsequently presented worsening swelling and eventually severely symptomatic superior vena cava (SVC)


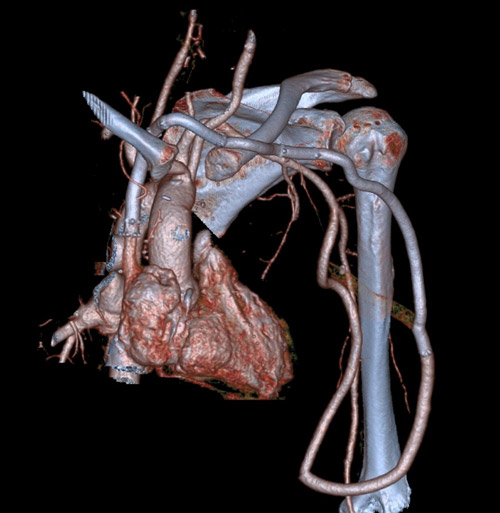
CAT Scan
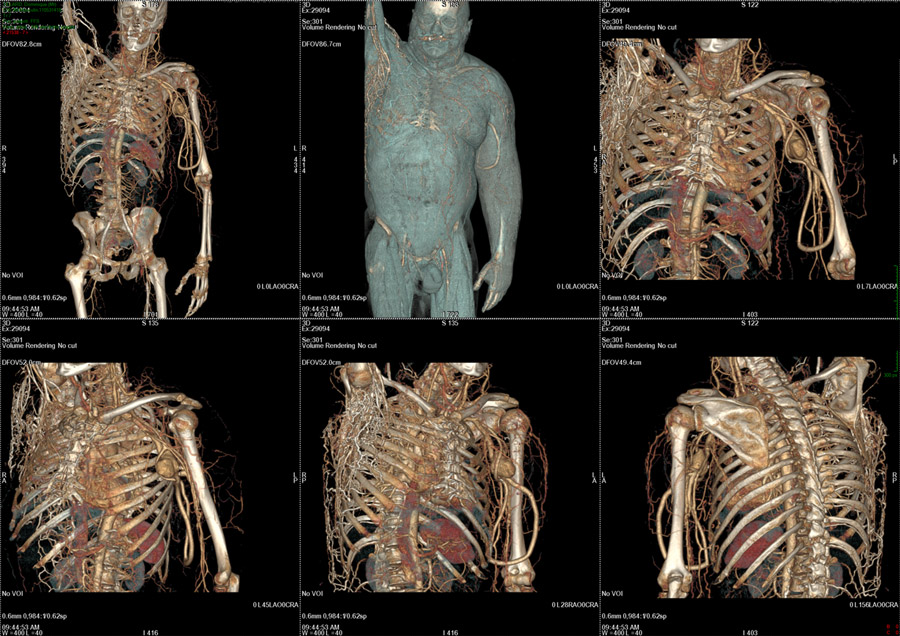
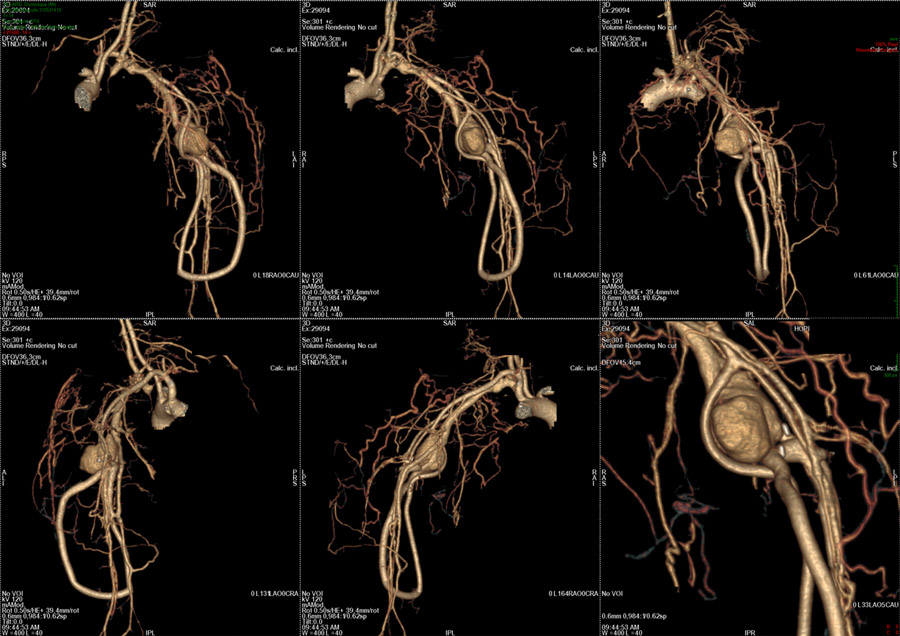
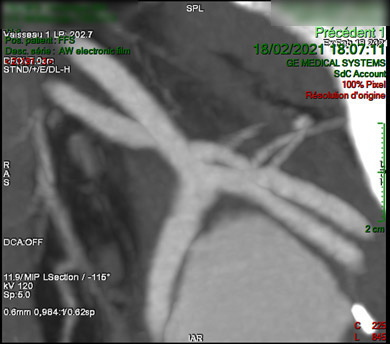
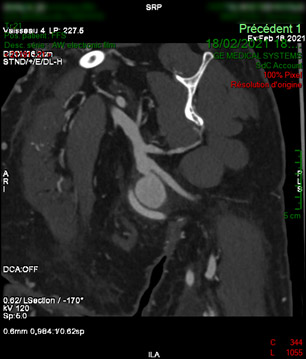

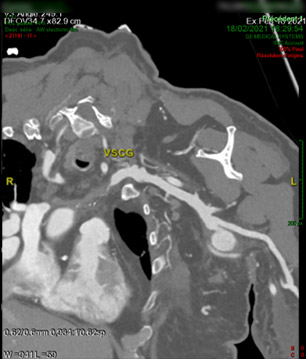
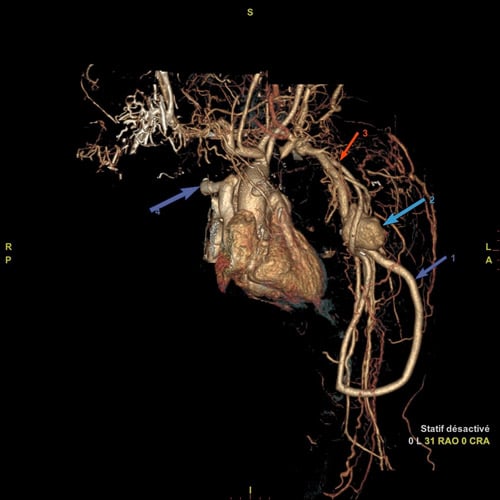
Interpretation
No venous outflow and patent used access created a context of high venous pressures:
- SVC Syndrome
- Venous anastomosis pseudoaneurysm
- Graft still being used albeit with difficulties of puncture due to oedema
- Relatively young patient with no other reliable access options
Recanalisation of left innominate vein was attempted but was not possible, a more imaginative approach was adopted...
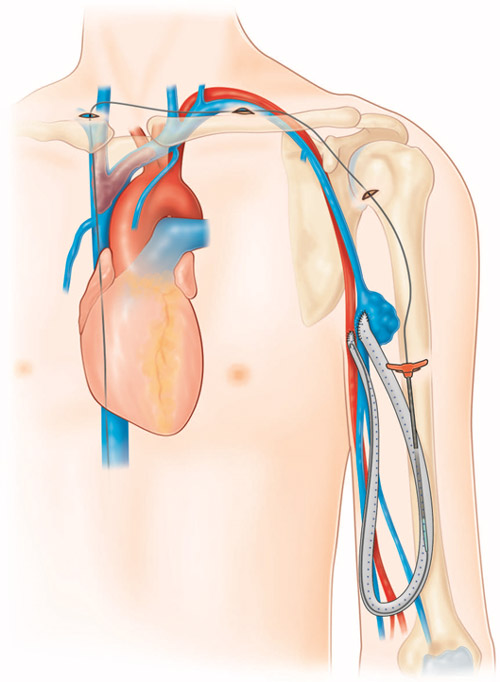
Endobypass between patent graft and SVC - Overview
- Surfacer device (Bluegrass, San Antonio TX – USA) was used to gain access
- Tunneled wire through subcutaneous space towards the left upper extremity graft
- Punctured graft with a peel-away sheath
- Got finally a unique stiff wire access connecting the right femoral vein through the patent SVC to the patent graft extra-anatomically
- Bridged with covered stents creating an extra-anatomical endo-bypass
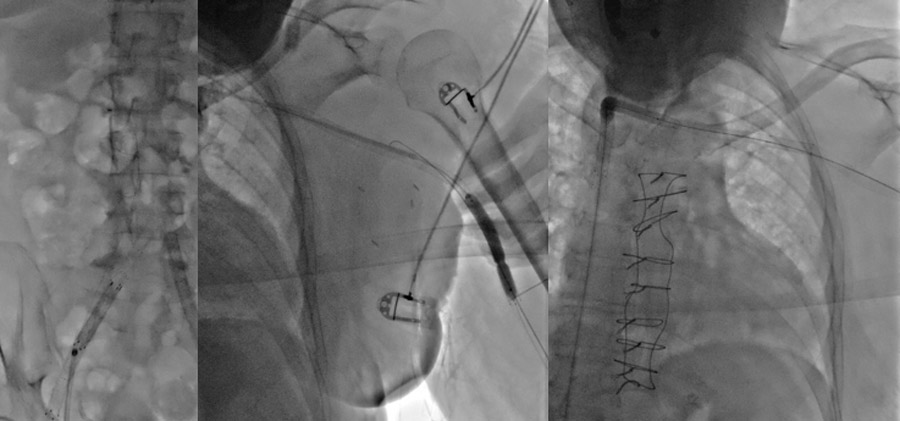
Intervention
Surfacer device was used to gain access through the femoral vein to the patent SVC, then through the occluded segment exteriorise a wire in a supraclavicular space

With the help of a snare a through and through access was created right femoral vein – SVC – right suprclavicular space – subcutaneous tunnel – AVG)
Covered stents were placed and post-dilated creating an endobypass between the used graft and the patent final segment of SVC

Case published: https://www.jvascsurg.org/article/S0741-5214(21)02209-6/fulltext
Get the latest clinical cases and breaking news delivered straight to your inbox!
