Aorta
Iliac / aorto iliac
Occlusive disease
Unilateral iliac artery total occlusion
A 67-year-old woman with extensive cardiovascular history presented with severe, lifestyle-limiting claudication progressing to rest pain (Rutherford III–IV).
Imaging revealed a total occlusion of the left common iliac artery, with distal refilling through collateral pathways with a patent hypogastric artery.
In such a patient with multiple comorbidities and complex anatomy, what is the most appropriate revascularisation strategy?

Leforte Hospital – São Paulo, Brazil
Part I - Case presentation
- A 67 year-old-woman, BMT + 🚭 🚬
💊 anti-hypertensive, statin, aspirin - Symptomatic claudication over very short distances / pain at rest – Rutherford III/IV
- 2 coronary stents, hemorrhagic stroke, cerebral aneurysm clipping (without sequelae)
- Cardiac status: grade I LV diastolic dysfunction. Aortic valve with incipient fibrocalcific degeneration.
- Normal spirometry, with no variation after bronchodilator administration (salbutamol spray 400 mcg)
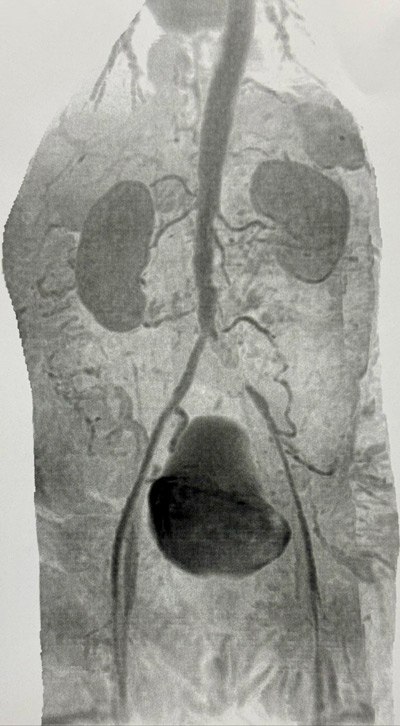
MRI: severe atheromatosis in all arterial segments with total occlusion of the left common iliac artery. Refilling of the external iliac artery by collateral and patent hypogastric artery.
Part II - Final strategy
Literature review to help determine the optimal treatment strategy
| Trial / Study | Reference | Key Findings |
|---|---|---|
| The COBEST trial | Durability of the balloon-expandable covered versus bare-metal stents in the Covered versus Balloon Expandable Stent Trial (COBEST) for the treatment of aortoiliac occlusive disease Mwipatayi BP et al. J Vasc Surg. 2016 |
The 5-year results demonstrated that the CS has an enduring patency advantage over BMS in both the short and long terms. The CS showed acceptable patency rates for more severe TASC C and D lesions, and patients who received a CS required fewer revascularisation procedures. However, the choice of stent did not affect the rate of major limb amputations. |
| Low-profile stents: midterm results | Midterm Results of Low-Profile Stents to Treat Atherosclerotic Iliac Artery Disease Troisi N et al. J Endovasc Ther. 2017 |
At 4 years, overall patency and absence of TLR were good. Midterm outcomes were poor in patients with Rutherford category 5/6 ischemia. The use of stents with a ≥ 6-mm diameter and postdeployment balloon dilation are recommended in all cases. |
| Covered stents for AIOD treatment | Covered Stents for Endovascular Treatment of Aortoiliac Occlusive Disease: A Systematic Review and Meta-Analysis Mallory A et al. Vasc Endovascular Surg. 2021 |
Covered stents are safe and effective for the treatment of AIOD. They were associated with a statistically significant higher odds of primary patency in both the overall cohort and in more complex TASC C/D lesions. Additional high-quality comparative analyses are needed to determine the most optimal treatment modality for AIOD. |
Percutaneous approach
- Left CFA puncture, 6F short sheath
- Unsuccessful retrograde recanalisation 18/35 GW, support catheter
- Left brachial puncture, 6F short sheath
- Exchange for long sheath 6F x 90 cm on left arm, positioned at distal aorta. Through-through technique
- Successful antegrade recanalisation 18/35 GW with SureCross™ (Merit Medical) support catheter
- Pre-dilatation POBA 6 x 40 mm and Tri-Wedge™ (BrosMed Medical) scoring balloon 8 x 60 mm (to prevent the stent detaching ‘crimp’ from the shaft)
- Exchange femoral 6F short sheath for 8F (compatible with stent profile)
- Gore* VBX balloon-expandable covered stent 8 x 59 mm
- Final angiogram: well-positioned patent stent, satisfactory remodeling, good contrast outflow
- Closure device on left femoral and brachial manual compression
1st post-surgical follow-up:
- 💊 DAPT Aspirin 100 mg + Clopidogrel 75 mg for 6 months
- Palpable pedal pulse (patient extremely satisfied, filling warm foot)

Statement of Financial Interest
Dr. Gustavo Aurelio Basso declares that he has no relevant financial relationships or conflicts of interest to disclose.
Get the latest clinical cases and breaking news delivered straight to your inbox!
