When complex intra-stent occlusion demands outside-the-box thinking
A 78-year-old haemodialysis patient presented with left upper limb swelling and loss of AVF thrill after multiple prior interventions on the left subclavian vein.
Imaging revealed complete intra-stent occlusion, posing a critical challenge for access preservation.
What would be your next step?




Our patient was a 78-year-old man with end-stage renal disease under haemodialytic regimen with a history of prostatic cancer and myocardial infarction
- 03/2023: Proximal arterio-venous fistula creation (brachio-cephalic)
- 01/2024: PTA of subclavian vein stenosis (1)
- 08/2024: Stenting of severe subclavian vein re-stenosis (2)
The patient presented at the end of July 2025 with oedema and swelling of the left upper limb in the absence of AVF thrill.
Vascular duplex ultrasound revealed a complete occlusion of the left subclavian vein stent.
Our choice was to perform an endovascular rescue of the vascular access.
The fistulography, performed via the cephalic vein percutaneous access, confirmed the stent occlusion (3) and suggested a possible misalignment with the central venous route.
The initial retrograde approach through cephalic vein puncture failed to cross the occlusion.
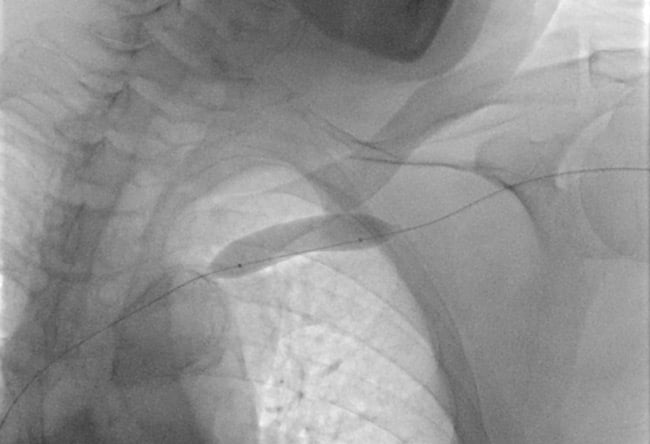
We then attempted a venous transfemoral approach, positioning a 7F, 65-cm introducer sheath with its tip in the superior vena cava.
Phlebography confirmed complete occlusion (4). Multiple catheters and guidewires were employed, but without success.
Strategy change:
We decided to perform an access in the left basilic vein to achieve a more favourable angle (5).
Using a 0.018” Halberd guidewire and a support catheter, we successfully recanalised the intrastent occlusion.
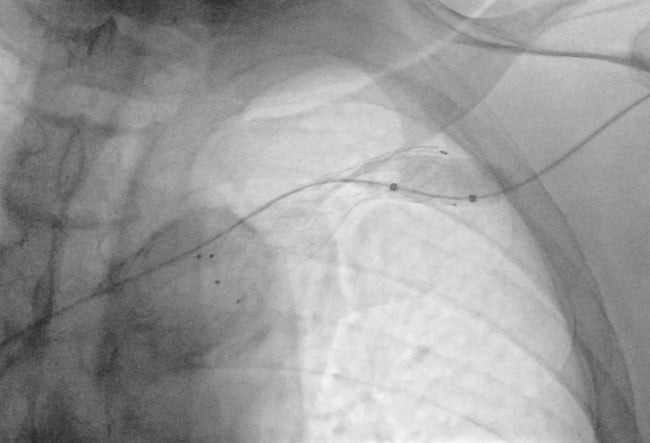
A snare catheter was used to establish a through-and-through access between basilic and femoral access (6).
With the through-and-through guidewire, we advanced the 7F introducer sheath from the femoral venous access inside the occlusion (7).
A second through-and-through wire was then placed (8), reaching the cephalic vein lumen, the distal target of our intervention.
Pre-dilatation with a non-compliant balloon (7 x 80 mm) was performed.
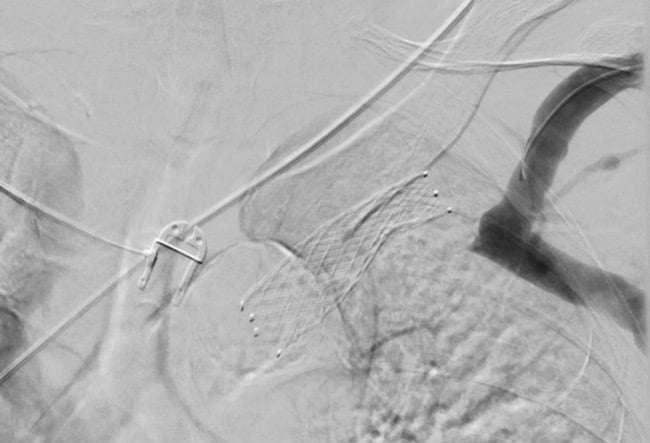
A self-expanding 16 x 60 mm stent was advanced (9) and deployed with sufficient overlap with the previous one onto the cephalic vein.
Post-dilation was performed with a non-compliant balloon catheter (14 x 40 mm).
Final phlebography shows the correct placement of the stent (10) and the satisfactory patency of the treated segment.
At the end of the procedure, a good thrill of the AVF was achieved.
Patient was relased from the hospital on the same day with single antiplatelet therapy.
At 6-month follow-up, fistula is still properly working ang the stents are patent.

Conclusion
This case proves how necessary it is to always consider alternative access routes and to show technical creativity in situations that require a specific approach tailored on the patient.
Get the latest clinical cases and breaking news delivered straight to your inbox!
