Acute limb ischaemia: comparing revascularisation strategies—ALIVE Registry insights
Selected in ESVS Journal by Mhamad Ali Hajj Hassan
Acute lower limb ischaemia (ALI) is a vascular emergency associated with high risks of limb loss and mortality, requiring rapid diagnosis and revascularisation.
While open surgery has long been the standard of care, endovascular and hybrid approaches have increasingly been adopted in contemporary practice. However, robust comparative data on their relative effectiveness and safety—particularly in real-world, multicentre settings—remain limited.
The ALIVE Registry was designed to address this gap by evaluating outcomes following different revascularisation strategies in patients presenting with ALI.
References:
Authors: Nikolaos Konstantinou, Dimitrios Vlastos, Athanasios Saratzis, Nicola Troisi,∙Mario D’Oria, Luca Bertoglio, Walter Dorigo,∙Gladiol Zenunaj, Angeliki Argyriou, Lukla Biasi, Michael Czihal, Georgios A. Pitoulias, Teresa Martín González, Manar Khashram, Pablo Del Canto Peruyera, João Ferreira Pires, Konstantinos Stavroulakis, on behalf of the ALIVE Registry collaborators
Reference: Published online January 20, 2026
DOI: 10.1016/j.ejvs.2025.12.060
Read the abstractObjective:
This study aimed to evaluate perioperative and mid-term (up to 3 years) clinical outcomes following revascularisation for acute lower limb ischaemia (ALI).
It compared contemporary treatment strategies—open surgery, endovascular, and hybrid approaches—using adjusted analyses to account for baseline differences between patient groups.
Study:
The ALIVE registry is a multicentre, retrospective cohort including patients treated across 20 centres between January 2016 and November 2024.
It provides real-world data on current revascularisation practices for ALI, with a focus on comparing outcomes between open, endovascular, and hybrid techniques using robust statistical adjustments.
Population:
A total of 1,259 patients with acute lower limb ischaemia (< 14 days) were included.
Treatment distribution was 56% open surgery, 20% endovascular, and 24% hybrid procedures, reflecting contemporary clinical practice across multiple centres.
Outcomes:
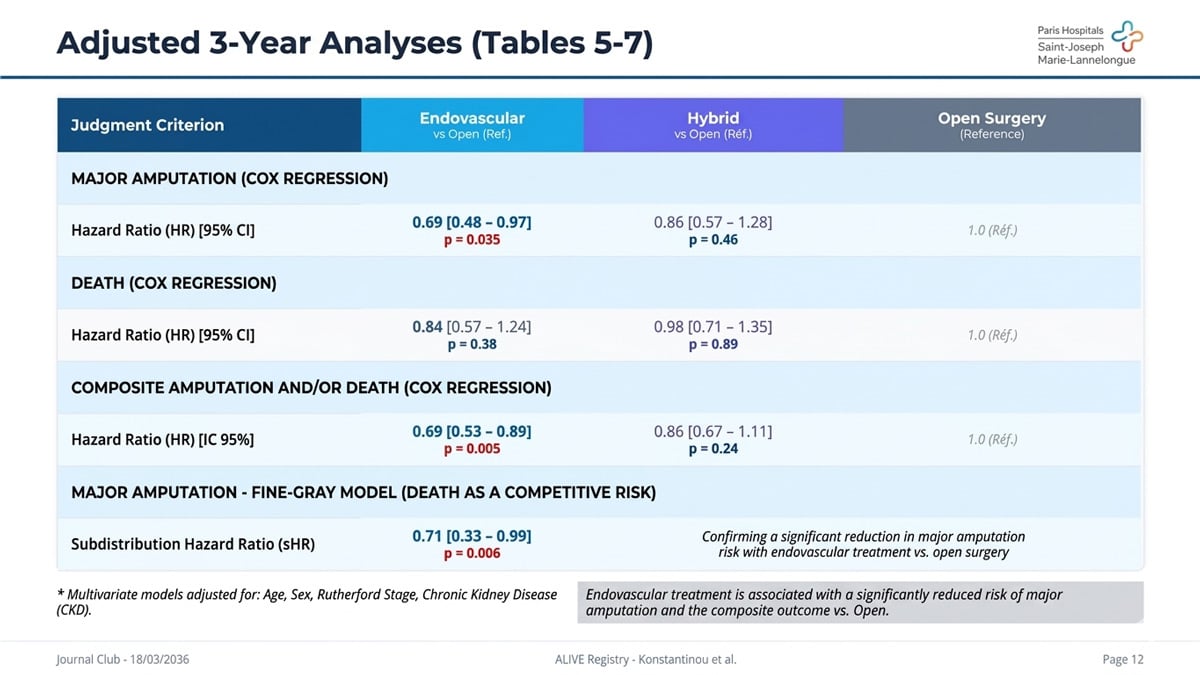
At 3 years, the endovascular approach was associated with a significantly lower risk of major amputation (HR 0.69) and the composite endpoint of amputation or death (HR 0.69) after adjustment. Overall survival was comparable across treatment groups.
At 30 days, mortality reached 11%, with lower early mortality and reduced incidence of acute kidney injury observed in the endovascular group.

Get the latest clinical cases and breaking news delivered straight to your inbox!

Conclusion:
Endovascular revascularisation represents a safe and effective alternative to open surgery in patients with acute limb ischaemia.
It is associated with improved limb-related outcomes and comparable survival, supporting its use as a first-line strategy in appropriately selected patients.
Discussion:
These findings support a shift toward less invasive strategies in ALI management, with endovascular techniques offering both perioperative safety and durable outcomes.
However, the observational design exposes the study to selection bias and inter-centre variability. While adjusted analyses strengthen the results, randomised controlled trials are needed to confirm these findings.
Careful patient selection remains essential, particularly in individuals with severe comorbidities such as chronic kidney disease.