Intermittent claudication: validation of SVS appropriate use criteria
Selected in JAMA Surgery by Miléna Usui
A multi-institutional study validates the SVS Appropriate Use Criteria (AUC) for intermittent claudication, showing that over half of revascularisations may be classified as inappropriate, particularly in patients with mild or moderate lifestyle limitations.
Inappropriate procedures were linked to lower 2-year freedom from reintervention and a higher risk of major amputation, highlighting the potential of the SVS AUC to reduce overuse and improve patient outcomes.
References:
Authors: Olamide Alabi, Rae Rokosh, Xinyan Zheng, Caitlin W. Hicks, Emily L. Spangler, Gabriela Velazquez, Kakra Hughes, Philip Goodney, Elizabeth L. George, Jialin Mao, Shipra Arya, Matthew A. Corriere
Reference: JAMA Surg - Published Online: December 17, 2025 - 2026;161;(2):161-169.
DOI: 10.1001/jamasurg.2025.5556
Read the abstractObjective:
The aim of this study was to perform a multi-institutional retrospective validation of the Society for Vascular Surgery (SVS) Appropriate Use Criteria (AUC) for management of intermittent claudication (IC).
Study:
Retrospective review of patients treated for IC from 2005 an 2024 across 7 institutions.
Population:
372 patients with IC who had a consultation with a vascular surgeons and met the original assumptions of the AUC.
Endpoints:
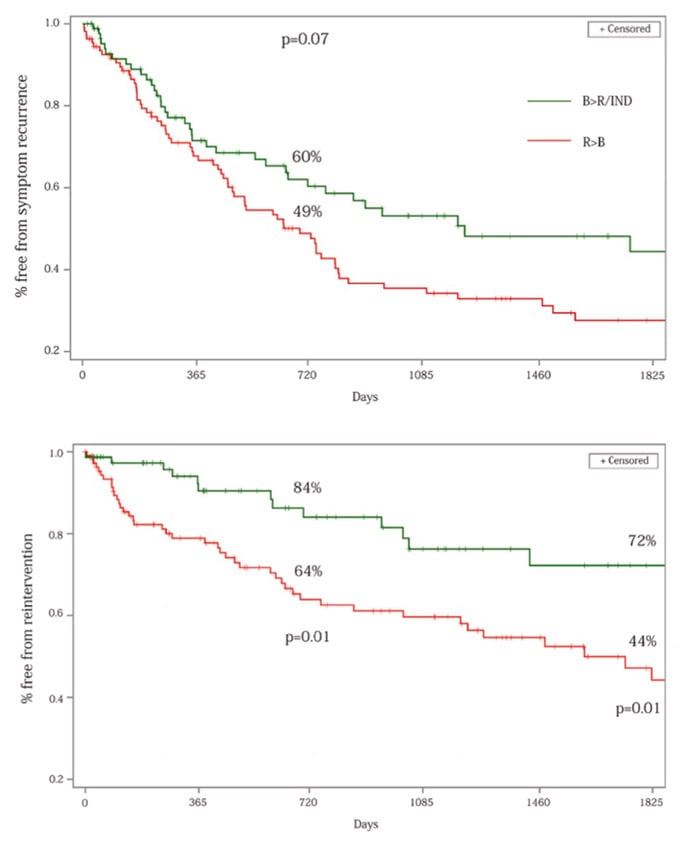
Freedom from invasive revascularisation, freedom from reintervention at 2 years, and freedom for symptoms recurrence.
Outcomes:
- Over a half of patients revascularised for IC were classified as R > B according to the AUC, driven primarily by femoropopliteal interventions in patients with mild or moderate lifestyle limitations.
- Retrospective classification of IC treatment by appropriateness according to the SVS AUC demonstrated significantly lower freedom from reintervention at 2 years post. Revascularisation in inappropriate vs appropriate/indeterminate
- Among patients who had mild/moderate lifestyle limitation and were classified as R > B, 10 major amputations occurred vs none in B>R/IND.

Get the latest clinical cases and breaking news delivered straight to your inbox!

Conclusion:
The SVS AUC has potential to reduce procedural overuse and minimize adverse outcomes in the management of IC.