A challenging growing neck mass
A 63-year-old man with an extensive history of left carotid surgery and a bovine aortic arch presented with a growing pulsatile neck mass.
Imaging revealed a sizable carotid aneurysm involving the distal CCA and ICA — an especially delicate scenario after multiple prior reconstructions.
With open repair deemed high-risk, the team faced the challenge of defining the safest and most durable strategy.
This case walks through the anatomical pitfalls, technical considerations, and the multidisciplinary reasoning that shaped the final approach, before revealing how the aneurysm was ultimately managed and how the patient fared.


Introduction
Carotid artery aneurysms are uncommon vascular pathologies, often associated with significant cerebrovascular embolism risk and a history of prior interventions.
Treatment remains particularly demanding and without guidelines when occurring in patients with multiple surgical reconstructions and concomitant anatomical variants, such as a bovine aortic arch.
We aim to present a complex case of repeat endovascular reconstruction for carotid aneurysm, highlighting technical aspects, decision-making, and early clinical outcome.
Clinical presentation
A 63-year-old male with hypertension, type II diabetes, hyperlipidemia, obesity, and peripheral arterial occlusive disease presented with a progressive pulsatile left neck swelling.
His surgical history included left carotid endarterectomy with patch angioplasty (2014), redo CEA with bovine patch (2021), contralateral right carotid eversion endarterectomy (2021).
CTA demonstrated a bovine arch configuration with the left common carotid arising from the brachiocephalic trunk and an aneurysmal dilation of the distal CCA extending into the ICA, measuring 1.6 × 1.8 × 3.5 cm.

After multidisciplinary discussion, endovascular repair was selected over open re-operation.
Via transfemoral access under local anesthesia, two overlapping Viabahn covered stents (5 × 50 mm and 6 × 50 mm) were deployed.
Due to the arch anatomy and prior reconstructions, embolic protection was deliberately omitted.
Perioperative antiplatelet management included aspirin plus a clopidogrel loading dose.
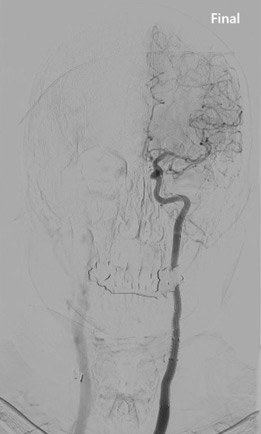
The procedure was technically successful, with complete exclusion of the aneurysm and preserved ICA perfusion.
Post-operative monitoring in the stroke unit revealed no neurological deficits.
The patient was discharged on dual antiplatelet therapy.
Follow-up duplex ultrasound at early control confirmed durable stent patency without endoleak or thrombotic complication.
Conclusion
Endovascular stent-graft reconstruction represents a safe and effective alternative to high-risk surgical reintervention in carotid aneurysm patients with prior operations and challenging anatomy.
This case underscores the importance of precise anatomical assessment, tailored device selection, and interdisciplinary planning.
Further multicenter registry data are warranted to establish long-term durability and efficacy of this approach.
Get the latest clinical cases and breaking news delivered straight to your inbox!
