Aorta
AAA
SYMPTOMATIC AAA post EVAR: Homemade FEVAR?
Considering the clinical evaluation and medical history of this 87-year-old patient with symptomatic AAA, suggest a treatment plan prior to uncovering the subsequent course of this case!

Hospital Pellegrin - Bordeaux, France
Professor of vascular surgery, PVI Editor-in-Chief
Professor of vascular surgery
Head of unit of vascular surgery CHU Bordeaux - France
Conflicts of interest:
Honoraria from: COOK Médical, Térumo-Vascutek, Siemens, GORE
Part I - Case presentation
- A 87-year-old male patient with HTN, Afib and hypothyroidism
- Biological aortic valve replacement in 2013
- EVAR for infrarenal AAA in 2015
- Atrial flutter ablation in 2020
He presented with symptomatic AAA with 2 cm diameter increase.
Part II - Treatment
Homemade FEVAR with 3 FEN
- TREO endograft modified by physician, who created 3 fenestrations for SMA and the two renal arteries
- In the emergency suite with motorized C-Arm and carbon floating table
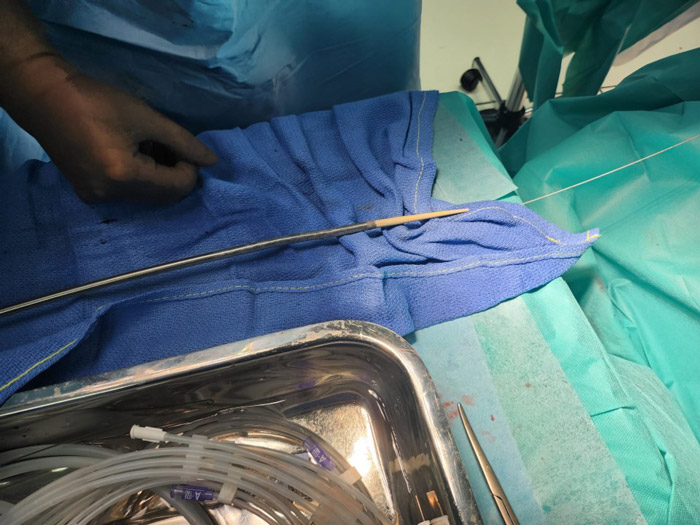
Stent-graft modification steps
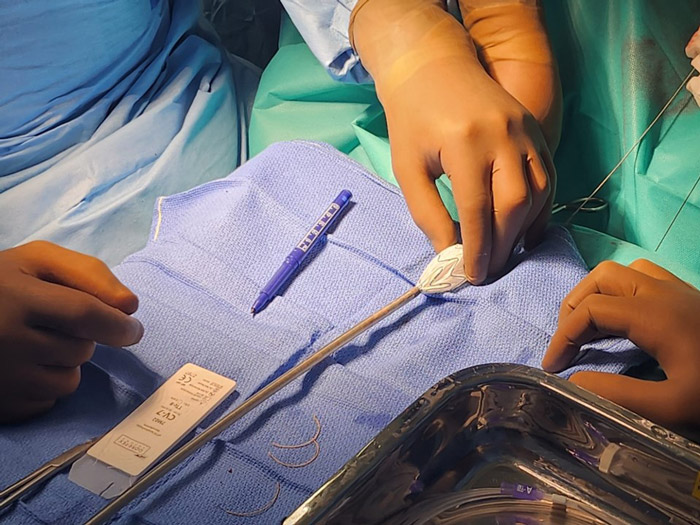
Opening of the proximal part of the endograft with sufficient length for fenestration shape

Fenestration marking in accordance with sizing

Fenestration creation with cautering pen
3 fenestrations created for SMA and both renal arteries

Lasso suture for circular reinforcement and radio visibility
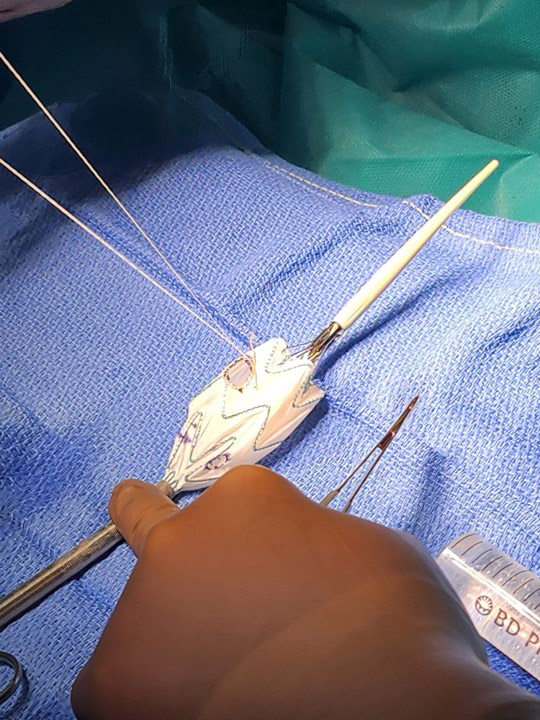
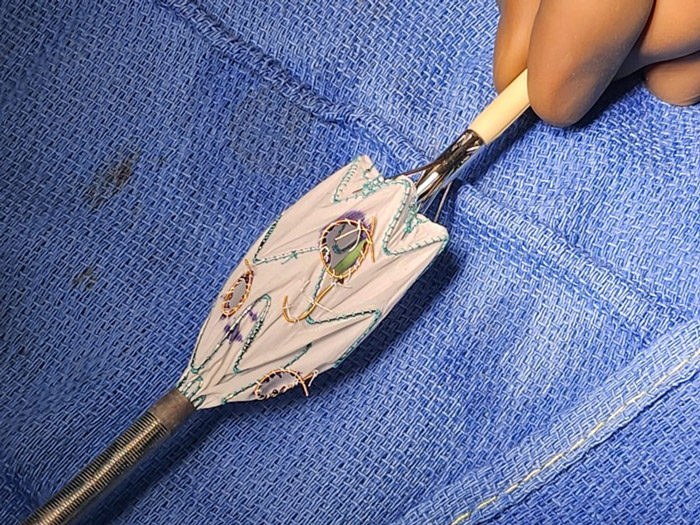
Anterior J-mark for optimal positioning and orientation
TREO PMEG with 3 implemented fenestrations
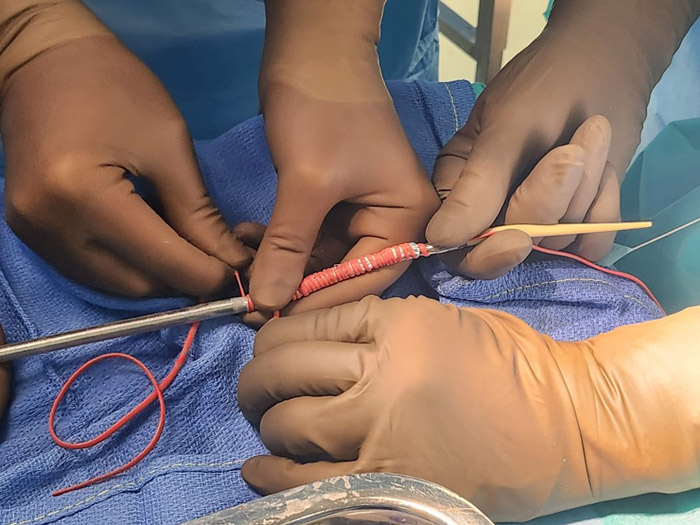
Graft reloading with elastic vessel loop
Initial angiogram - SMA and both renal arteries individualization
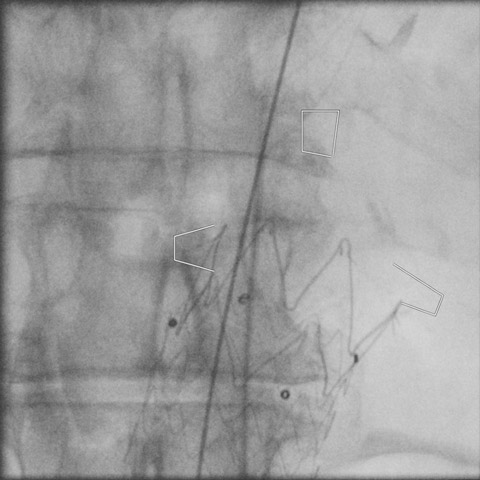
Target vessel marking
PMEG endograft: delivery and positioning
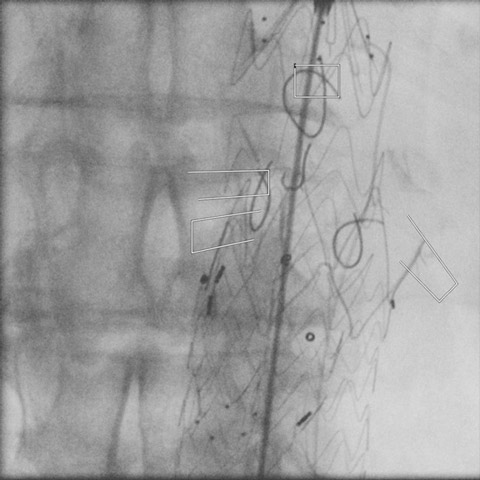
Right renal cannulation
Left renal cannulation with UF catheter and 0,035 guidewire
SMA cannulation with Vanchie 3 catheter (Cook Medical, Bloomington, Ind) and Rosen guidewire (Cook Medical, Bloomington, Ind) delivery
7 Fr sheath for SMA and angiogram control after 7 x 37 covered stent delivery. Note the 2 renals stented with 6 x 37 and 6 x 27 iCover covered stents ((iVascular)
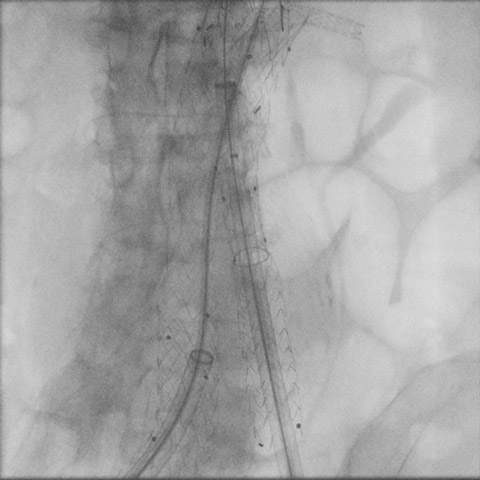
Leg adjunction on both sides for perfect exclusion and distal stability.
Post-op
- Uncomplicated
- Discharged on PO day 5
Get the latest clinical cases and breaking news delivered straight to your inbox!
