Treatment of recurrent endoleak type II
Type II endoleaks after EVAR are usually harmless and often resolve on their own. But in this case, an 80-year-old patient faces a stubborn recurrence: his aneurysm sac continues to expand despite previous interventions.
Follow this case to understand the challenges of identifying feeding vessels, planning embolisation strategies, and deciding when further treatment is warranted.

Introduction
- Type 2 endoleaks (EL2) after EVAR are common with self-limiting behaviour in most cases.
- According to current guidelines, treatment is conservative. The intervention is indicated only with expansion of the sac ≥ 5mm.
- Different approaches for embolisation have been used and, despite high technical success, recurrence is not uncommon and many patients require multiple interventions.

Clinical presentation
- Our patient is an 80-year-old male.
- Medical history:
- Atrial fibrillation
- Hypertension.
- Ischemic heart disease.
- COPD
In May 2022: EVAR for a 52 mm infrarenal AAA with Ovation ALTO and right renal polar embolisation.
In October 2022: follow-up with EL2 and sac growth (57 mm).
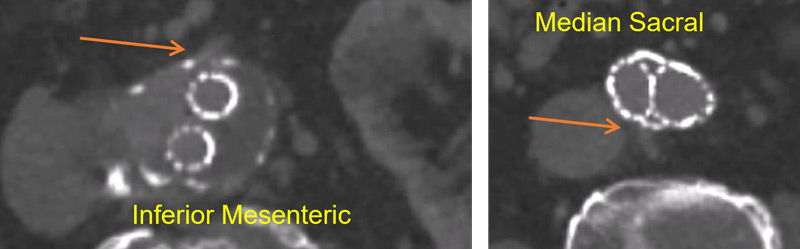
In July 2023: angiography with selective catheterisation of the superior mesenteric artery, without identifying contact with the Arc of Riolan or direct connection with the inferior mesenteric artery.
Right hypogastric catheterisation, identifying branch that connects with median sacral, without being able to catheterise it.
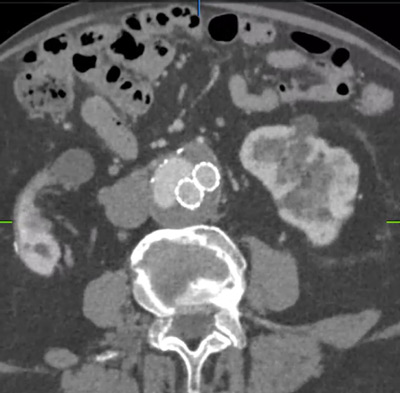
On angio-CT 2024: persistence of EL2, with sac growth (59 mm).
- Sac growth.
- Correct sealing.
- Endoleak lateralised to cava
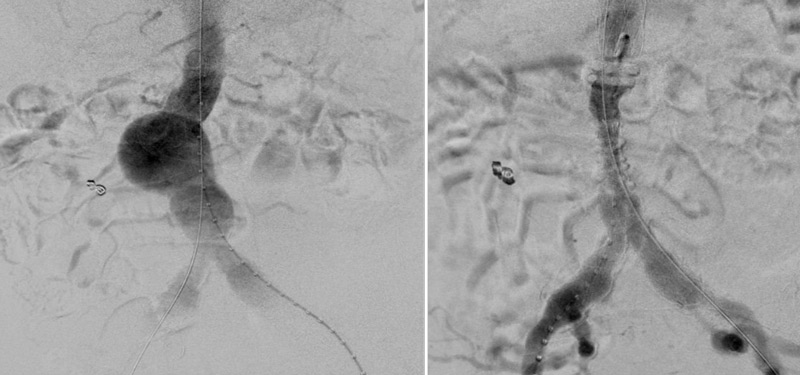
Transcaval embolisation (TCE)
- Right common femoral vein puncture (TCE)
- Left common femoral artery (control arteriograms)
- Left internal saphenous vein (IVUS guidance)
- Transcaval access
- Embolisation of the sac and afferents
Follow-up CT
Take-home messages
- Transcaval embolisation provides an alternative strategy with success rates comparable to other techniques.
- It can be an advantage when the endoleak is on the right side of the sac and/or in recurrent endoleaks.
- Preserving entry to the sac is essential in this type of endoleak.
Get the latest clinical cases and breaking news delivered straight to your inbox!
